Making Cancer Prevention Work for Everyone
February 24, 2026

Cancer prevention is often framed as a shared responsibility that depends on individual behavior, clinical guidance, and system readiness. We encourage people to eat well, stay active, and follow recommended screening schedules, making early detection as essential to better outcomes. Each February, National Cancer Prevention Month reinforces these messages.
Yet for millions of people with disabilities, cancer prevention is not always designed with their needs in mind.
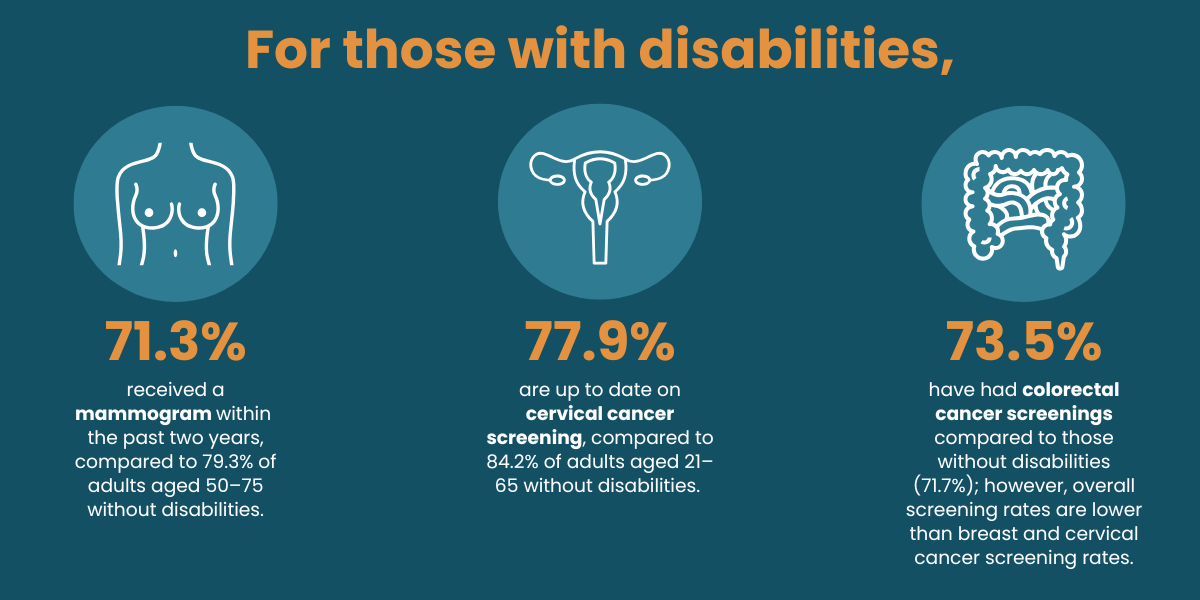
Adults with disabilities in the U.S. experience higher rates of cancer than adults without disabilities. This disparity does not stem from a lack of awareness or motivation, but from structural barriers that shape how prevention guidance is delivered, understood, and acted upon. When prevention strategies assume that everyone can move, communicate, process information, and tolerate clinical procedures in the same way, access becomes uneven by design.
This is not a marginal issue. It is a signal that our prevention frameworks, however well‑intentioned, have not fully caught up with the lived realities of many people.
Missing the Mark
Traditional cancer screening guidance often reflects an unspoken norm: that patients can stand independently, maintain specific positions, follow complex written instructions, and navigate healthcare settings without additional support.
In practice, many screenings challenge these assumptions. Mammography frequently requires standing and remaining still during positioning, creating barriers for people who use wheelchairs or who experience pain, fatigue, spasticity, or sensory sensitivities. Colorectal cancer screening often involves detailed, multistep bowel preparation instructions that rely heavily on dense written materials, which may not meet the needs of people with intellectual or cognitive disabilities.
Recent research shows that incomplete colonoscopies are more common among people with intellectual disabilities, suggesting the problem is not noncompliance, but whether instructions and supports are accessible and usable in the first place. When screenings are difficult to complete, or not offered at all, the consequences are predictable: delayed detection, missed diagnoses, and preventable inequities.
Accessibility Begins with Communication
Improving access to cancer screenings does not always require new technology or specialized equipment. Often, it begins with communication.
Clear communication before a screening is scheduled can fundamentally change the experience for the better. When healthcare professionals explain what will happen before, during, and after a screening, including what abnormal results may mean, patients are better positioned to identify needed accommodations and make informed decisions.
Step‑by‑step explanations delivered in accessible formats are not ‘extra;’ they are foundational, reducing anxiety, supporting preparation, and allowing patients to engage as active partners in their care. When communication improves, trust follows, and trust is essential to effective prevention.
From Awareness to Action
Recognizing disparities is only the first step. The real challenge for health systems is translating awareness into everyday clinical practice.
Evidence‑informed resources, such as Screening for All, demonstrate that disability‑inclusive cancer screening is both achievable and practical. By supporting clinicians with decision‑making tools, plain‑language patient resources, and implementation guidance, these approaches integrate accessibility into routine workflows rather than treating it as an exception.
A Broader Definition of Prevention
National Cancer Prevention Month invites an important question: prevention for whom?
Cancer prevention is most effective when recommendations are achievable for all patients and when health systems are prepared to meet people where they are. Inclusion is not a separate initiative. It is a measure of quality.
Designing prevention for accessibility does not narrow our reach — it expands it. In doing so, it moves us closer to a prevention system that works for everyone.
This program is supported by the U.S. CDC of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $974,773.00 with 100% funded by CDC/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by CDC/HHS, or the U.S. Government.